LEADER IN THE NEUROTECH SPOTLIGHT: ALEX WOODS, CO-FOUNDER AND CEO, NEWROTEX

ABOUT LIZ MOYLES, HEAD OF NEUROTECH – AUTHOR

A self-described frustrated neurosurgeon, a lengthy hospital stay in her teenage years left Liz with PTSD and a fear of hospitals and blood, rerouting her path at 18. Medicine was the plan. Biochemistry became the reality. But life in a lab was not where she belonged. What never left her was her fascination with the brain and the people building in the space.
Today, as Head of Neurotech at Cruxx, she works with start-ups and scale-ups across the US, Europe and beyond to help them attract the talent and capital required to build.
Her aim is simple: to give CEOs and leadership teams their time back to operate at a strategic level, not get pulled into day-to-day execution.
Fundraising, clinical trials, and regulatory work already stretch teams thin. Hiring sits on top of all of it. When it goes wrong or moves too slowly, the consequences are immediate. It can mean missing funding, delaying submissions, slipping milestones, or losing people through overload.
Liz leads global executive searches for VCs and neurotech companies, placing C-suite and board-level leaders and building out senior teams across the US, Europe and beyond.
Embedded in the neurotech ecosystem, she speaks regularly with founders, operators, KOLs and investors, giving her a clear view of where the field is heading and what it takes to succeed in a start-up. That perspective shapes how she approaches hiring.
In start-ups, every hire matters, and attracting the best is non-negotiable. But they are rarely looking. Busy building elsewhere they are often unaware of what you’re doing.
Finding them is one challenge. Getting them to engage is another.
But while you and your hiring managers are trying to find these people, the clock is running. FDA submissions, fundraising rounds, clinical trials. Everything that cannot wait………. is waiting.
That person is out there. Liz knows the space and where to find the people.
They just don’t know you exist………….. Yet!

A HOSPITAL WARD IN COVENTRY, UK
Dr. Alex Woods has spent his career with his hands inside the human body.
As a trauma and orthopaedic surgeon at Oxford University Hospitals, he has seen more than many people ever will. The sharp end of catastrophic injury. The long road to recovery- and sometimes the moments when medicine has run out of answers to a patient’s condition.
It is that last part that stayed with him and eventually led to Newrotex, the company he co-founded. The team are developing the only treatment of its kind in the world, that I know of to treat the “heart sink” cases relating to peripheral nerve injuries.
These are the ones where even the most experienced consultants look at the patient and say, with no drama and no apology, that they will face a grim future. Not because anyone has failed. But because the system has nothing truly effective to offer.
Every year sadly there are 1.5 million operations for nerve injuries.
The standard treatment for a large gap nerve injury is autografting which often results in a second injury and involves long surgery times, along with risking donor site morbidity and infection.
Removing a healthy nerve from elsewhere in the patient’s body to fill the gap. It causes guaranteed harm in one place to attempt repair in another.
-If the gap is more than 3cms, efficacy drops below 40%.
-Past 5 cms, it falls to around 9%.
-That is the gold standard.
Alex did not set out to be a founder. He set out to be a surgeon. But before medicine, he studied Human Sciences at Oxford, then completed a DPhil in Zoology, and worked as a postdoctoral researcher studying the material properties of spider silk with Professor Fritz Vollrath, one of the world’s leading silk biologists.
The connection between those two worlds did not arrive as a flash of insight. It arrived the way most real ideas do. Gradually, then suddenly. In a hospital ward in Coventry, watching a consultant confirm to a patient with a serious nerve injury that there was nothing to be done.
That moment would not leave him.
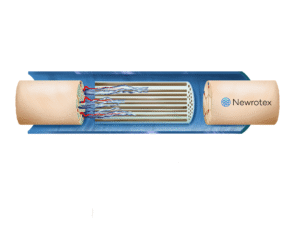
Newrotex, the company he co-founded with Professor Fritz Vollrath, is developing SilkAxons®, a patented implant made from spider silk fibres that guides nerve regeneration across gaps of up to 10 centimetres.
That is more than triple the reach of any device currently approved by the FDA.
It requires no donor nerve. It stores at room temperature. And its first-in-human trial, launched in 2025, has already returned results that no one in this space is taking lightly.
– 5 patients. 8-10cm nerve gaps.
-All 5 regained sensation. None feel any pain today.
-One patient, who after having a large nerve tumour removed from his thigh, was told he might never walk again, is walking.
In January 2026, the BBC came to Oxford to film inside the Newrotex laboratory. 30 golden orb-web spiders from Madagascar, each in their own terrarium, each producing the dragline silk at the heart of this story.
Alex is still a practising surgeon. He sees many patients -not just those with peripheral nerve injuries but it is this population that concerns him the most. Like other surgeons he feels at a loss to help and that science is letting them down.
That dual identity of founder and clinician runs through everything Newrotex is building.
The sad story here – is Newrotex is running out of funding and this may mean those 5 patients are the only ones they will ever be able to help.
SQUARE PEG, SQUARE HOLE
Liz: Let’s start with how you ended up as a practising surgeon and founder. Did you ever imagine this would be your destiny?
Alex: Not at all. Convoluted roots.
I studied Human Sciences as an undergraduate at Oxford, then did a DPhil in Zoology, then went to medical school. When I was a post-grad, I worked as a postdoctoral researcher studying the material properties of spider silk with Professor Fritz Vollrath, who is one of the world’s leading silk biologists, before becoming a trauma and orthopaedic surgeon.
The connection between the two worlds– the medical world and the world of medical devices did not arrive as a flash of insight.
It arrived the way most real ideas do. Gradually, then suddenly.
It was during my trauma training that we started seeing patients come through with serious nerve injuries. These are the “heart sink” patients. They do not do well. Recovery is very unpredictable, often quite poor.
Liz: Can you tell me a bit more about this and “heart sink” cases. What do you mean by this?
Alex: Yes, roughly 1.5 million people have a peripheral nerve injury each year. We got to a point where we were seeing a lot of patients with nerve injuries bigger than 3 cm sometimes – sometimes up to 10 cm.
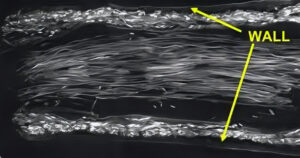
A nerve is like a fibre optic cable. A tube with little wires down the middle that transmit information. If you cut a nerve, it pulls apart and it cannot regenerate on its own beyond a certain length.
The issue is peripheral nerves regenerate at roughly 1 mm per day, but only if a guidance structure / a scaffold is in place. The body forms temporary scaffolds, known as Bands of Büngner, but these begin to lose integrity within 10 days.
That means it can support nerve growth of circa 10mm maximally. So, you can see the issue we have – in larger nerve injuries the nerve effectively runs out of guidance before it reaches its target destination.
All the nerves really need is a scaffold to bridge across.
With my biomaterials background from my time as a zoologist, and from working with Fritz Vollrath, I realised between us we had something that could potentially address the ‘scaffold’.
So Newrotex was not born out of a beautiful mind moment.
It was literally, a case of “I’ve a square hole”, (patients with large nerve injuries), and we realised we had the “square peg”, (silk).
THE ROSE TRELLIS – 2 WORLDS COLLIDE!
Liz: So, it was pure serendipity. You were not looking for a problem to solve. You had a material and a clinical reality, and eventually they found each other.
Alex: Exactly. And I think that is how a lot of the best ideas in this space happen.
Fritz used to make all his students go to the bar near the building every Friday afternoon at four o’clock.
He would say, you are never going to have your great epiphany staring at a laptop for another two hours.
Go and have a drink. Meet someone two doors down. Have a chat about your problems.
You may realise they have got the answer. It may come from a different field, but the case could be that no one has ever combined it with your problem before.
Two worlds can collide.
That is genuinely how a lot of breakthroughs happen.
Liz: I agree. I was speaking with David Veino, CEO of Neuros Medical, we ran a Leader in the Spotlight feature recently and he had a similar story to tell. Neuros had a square peg. When he joined the model was to fit the peg into a round circle. With his background he quickly identified the square hole they needed to target. And the rest is history.
Tell me about the silk and Fritz. He is your co-founder. How did that relationship develop into Newrotex?
Alex: Silk is a natural material and the way we are using it is to do the same as the bands of Büngner but our silk lasts 150 days- not 10 days.
This means that when you lay it across the gap, caused by the nerve injury, suddenly the axons have the time to grow along it like a rose along a trellis. The silk dissolves. And that is it. You recover the nerve.
Fritz Vollrath leads the Oxford Silk Group at the University of Oxford. He is one of the most respected silk biologists in the world. He has decades of research and work on spider silk and its properties. He holds an MSc in Neurobiology and has founded several companies around silk technology, including Oxford Biomaterials, which was spun out of Oxford University back in 2001.
As I said, I worked in his lab as a postdoc. That is where the foundation for Newrotex was laid- not just scientifically but personally.
He and I stayed in touch as I went through medical school and surgical training. I acted as an adviser to Oxford Biomaterials along the way. The idea for Newrotex grew out of those ongoing conversations. Slowly. Over years.
It was never one moment. It was two people with complementary worlds, staying in the room together long enough for the right question to appear.
WHEN DOCTORS STOP TALKING ABOUT IT
Liz: Can you tell me about the moment this stopped being an academic question and became something you had to pursue?
Alex: Yes. I’ll never forget the moment. I was in my core surgical training, working at a big trauma hospital in Coventry.
Suddenly, it appeared that we were seeing case after case, after case of patients with significant nerve injuries. One day on duty with my consultant, I listened as he told a man that he would have to live with life-changing injuries and that he would never recover.
In fact, the prognosis may get worse.
I clearly see that man’s face still today. And I can also see the face of my consultant. The mixed emotions: sadness, disappointment, and a feeling of inadequacy -of not being able to offer any alternative solutions beyond what had already been offered.
I vividly remember how I looked to my consultants, expecting them to have an answer. They didn’t.
It was then I realised – there is literally nothing we can do. Science just hadn’t gone far enough.
The stark reality of it troubled me. But something deeper than that began bothering me – I started to realise something about how doctors act.
If there is a problem we cannot fix, we stop talking about it.
It falls out of the complications list. It becomes endemic in the culture that patients with these injuries just do not do well. We accept it.
That is sad.
I kept coming back to the anatomy of a nerve, and thinking “this should be straightforward. It is designed to try to heal. Why are the outcomes so bad?”
And then an idea began in the back of my mind. I spoke with Fritz. We started looking at what silk could do in this space, if anything.
PLUGGING A GAP AND OPENING ANOTHER
Liz: Alex, before we talk about the solution, take me through what is currently available. What are surgeons working with for large gap nerve injuries?
Alex: Currently, if you suffer a large gap nerve injury, we cut a nerve out from somewhere else in your body and move it to fill the gap. Autografting.
You get 100% morbidity because you are going to lose one nerve.
We are robbing Peter to pay Paul or plugging a gap but opening another.
Usually, we cut a nerve from your leg, the one that supplies sensation to a part of your foot.
25% of patients then develop chronic problems at the donor site. Painful neuromas. Lost function.
And as I said before, if the gap being repaired is more than 3 cms, efficacy drops to less than 40%. Past 5cms, it drops even as low as 9%.
So, we are putting a patient through all that knowing it probably won’t work but we have few other options.

30 SPIDERS FROM MADAGASCAR
Liz: Take me into the lab. What does the process actually look like?
Alex: We currently have 30 golden orb-web spiders at the Wood Centre for Innovation in Oxford. Each one lives in her own terrarium. We keep the room warm and humid to replicate their native Madagascan habitat.
To harvest the silk, we gently lay the spider on the back and reel the dragline silk from her, which they are naturally producing as they walk, so a colleague of mine in the silk world likens it to “taking the spider for a walk”.
It must be collected in a controlled, sterile way to meet medical device standards. Each spider can produce up to 4kms of silk in her lifetime, enough for roughly 20 implants over 6-9 months.
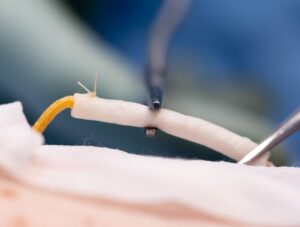
SilkAxons is a bundle of those silk fibres. The surgeon threads them through either a hollow conduit or a section of the patient’s own vein, then sutures the assembly across the nerve gap. The axons grow along the silk. The silk dissolves harmlessly.
What you are left with is a natural, regenerated nerve. No hardware. No second wound. Nothing to remove.
Liz: And what results have you had?
Alex: The nerve gaps we treated in our first-in-human trial were between 8 and 10 cms. These were injuries that under current standard of care would have resulted in permanent loss of function. The other thing that matters for accessibility to patients globally is that silk stores at room temperature.
No freezers. No cold chain.
That changes the economics for hospitals without the infrastructure for expensive cold storage.

THE CONSEQUENCES WE DON’T DISCUSS
Liz: Alex beyond peripheral nerve injuries can you see other applications.
Alex: The trauma cases are the obvious ones. But the applications go further than that. Much further. And this is one of the things that does not get talked about enough.
The trauma injuries, motorbike accidents, hand injuries, those are the cases surgeons worry about openly.
But there is another whole category. The nerves that surgeons damage every day doing one procedure that leads to further consequences we can neither avoid nor fix currently.
And because we cannot fix them, we do not talk about them enough.
Women who have mastectomies for breast cancer often lose sensation when the breast is reconstructed. The nerve tissue within the breast is removed along with the cancer. You can reconstruct the skin. You cannot give the sensation back.
There is a process where you try to reconnect a nerve from the chest wall to the nipple, but historically the gap has been too large to bridge reliably.
Our product can bridge those gaps. We could give women protective sensation back to their breasts after mastectomy.
And prostate resections. Bladder and rectal dysfunction after prostate surgery is nerve damage. The inability to repair those nerves is the problem.
Dental extractions that damage facial nerves. There are quite a few areas of the body where nerves are damaged because of surgery, and because we cannot fix them, we have stopped considering the possibility of a solution.
Liz: It’s a bigger TAM, therefore. I have had breast cancer myself. I know the consequences of surgery, chemotherapy & radiotherapy. They are the necessary evil to survive, but it hurts – to suffer more, than just the cancer itself. Especially when you may already be feeling bruised, battered and maybe disfigured.
Alex: Yes, breast reconstruction is a huge opportunity.
We have many KOLs in breast reconstruction who are genuinely excited about what this could mean. These women have already been through something life changing.
The nerve damage is a consequence that too often goes unaddressed because there has been nothing to offer.
Yes, we are saving lives, but it comes at a cost. It is always the least cost we can possibly get away with, but it usually comes with effects. It should not be that way.
5 LUCKY PATIENTS BUT THIS COULD BE THE END
Liz: Tell me about the first-in-human trial. What happened?
Alex: We launched the study in 2025, working with a CRO in Latin America. Regulatory approval came through just two weeks after submission which is in itself a huge indicator.
Five patients. Four of them had donor site nerves, the ones that would normally be sacrificed and left permanently without sensation.
All four have got sensation back. They would have had numb feet for the rest of their lives. Now they do not.
The fifth patient was told before the procedure that he would probably not walk normally again. He had a large tumour in his leg that would have cost him the use of his ankle and his foot. He has had it repaired with our implant. He is already walking again. Wearing shoes. Pushing off.
He does not need a calliper.
And not one of them has chronic pain. We expected up to 20% to develop chronic pain from the donor site. None of them have any at all.
The BBC covered our work in February 2026 and since then I get emails from members of the public asking to join the trial. When we were recruiting for this first study, patients were pre-enrolling themselves. Telling us they did not want surgery until we had approval, because they wanted the chance to have their nerve repaired rather than just be left to face a life with injuries that they would never recover from.
If you are a patient and someone says, I am going to cut this nerve, but it will lead to these problems later, OR there is a trial taking place where maybe that will not happen, that is not a hard decision.
Liz: I think the story of Helen is worth sharing here. Tell me about Helen.
Alex: Helen is Helen Hide-Wright. In 2022 she suffered a cardiac arrest at the wheel, crashed into a lorry, and broke almost every bone in her body.
Her right arm nerves were severed. Surgeons had to remove donor nerves from behind her foot to repair them.
Her foot is permanently without sensation as a result.
Her treatment was excellent. Exactly what the standard of care could offer. She has spoken publicly about being grateful for what she received.
But she now sits on our trial steering committee as an independent patient reviewer. She reviews our data. And she has said publicly that what we are building would have given her a better outcome.
She would not have lost the sensation in her foot.
That is the whole story, really.
The current gold standard harms patients to help them. Helen experienced exactly that trade-off. And she is now investing her time to make sure the next person in her position does not have to make the same choice.

OPERATING WHILST WONDERING IF I CAN MEET PAYROLL
Liz: Let’s talk about next steps
Alex: As a startup fundraising in the current environment, we know we could run out of money this year.
In the next 6 months. We may not find the financing we need.
But I can sleep knowing that there are 5 patients who have nerve recovery that would not have happened otherwise.
No one can take that away.
That is five years of work. It is not the way I want it to end. But you can’t put a price on that.
Liz: I find that so truly sad. How do you hold all of that when you walk into the O.R. and see yet another “heart sink” patient?
Alex: It is an emotional rollercoaster. There is no other way to describe it.
One morning you are on the BBC.
The next you are in a pitch trying to project conviction to an investor, and to your team, while doing the mental arithmetic of how long the runway lasts.
In the early years it was even more immediate. If our grant did not get paid that week, I could not pay anyone’s salary on Friday.
That is not something you want in the back of your mind when you are about to go into theatre.
The frustration is real.
We could have been 2 years further along if capital had come in earlier.
Every time you slow things down to conserve cash, you are making a choice that delays patients getting access to something that already works.
Liz: Implantable devices compete for investment against digital health and AI tools with very different cost structures. That must make the conversation harder.
Alex: That tension does not get talked about enough.
Investors who understand pure tech look at our numbers and see risk everywhere.
What they sometimes do not see is that the clinical evidence is already there, the regulatory path is mapped, and the strategic interest from large partners is real and at president of surgery level.
Not early conversations. Advanced ones.
But none of that pays salaries this week.
I sit in investor meetings and watch people get excited about a piece of software that costs $200K to put on the market, and I think, with my surgeon hat on, that is a harder clinical sell than people realise. But it is an easier investment story.
We still need development of implantable medical devices to drive standards of care forwards and therefore people who understand what they are backing and back it anyway.
Liz: What would change that picture for you?
Alex: Getting this round closed. Getting the pivotal study started. Getting more implants into patients in the UK and the US.
We have just submitted our FDA Breakthrough Device Designation application.
We meet all the four criteria. That hopefully changes the regulatory timeline and the investment conversation significantly if it comes through. Once we have the pivotal data, the story becomes much harder to ignore.
The strategics already know it. The market is there. Axogen has spent years building it, and they have done important work.
But the large gap problem is still unsolved. That is the opening.

THE SURGEON IN THE ROOM
Liz: How does being a practising surgeon impact your decisions as a founder?
Alex: I can hold my hand up and say I am an end user. When anyone asks whether surgeons will care, I care. I am one of them.
It opens doors when I am talking to KOLs and to peers. They know they are talking to another surgeon, not a founder or startup trying to sell them something. That changes the quality of the conversation.
It also helps with trial design, quality systems, understanding what end users need from a device in a real clinical setting.
The flip side is real though.
Surgical training gives you expectations about performance and working hours that are not realistic for a startup. You have to unlearn a lot of that as a CEO. And the NHS gives you a very warped view of what a reasonable salary looks like(!)
Liz: Tell me Alex, how do you establish what surgeons may truly value when developing your solution? Are there any insights you can share?
Alex: I respect the work of KOLs. They are champions but the person with the biggest name might have that name precisely because there has been no solution to the problem. They are the expert in managing something we cannot fix. That is a different thing from being the right voice to champion something new.
What I think you really want is not just a key opinion leader.
You want a key clinical leader. Someone engaged in development early, giving you the insight to fix the problems before the technology is ready to launch, so that when it is, the most senior people in the room have already had their questions answered.
You do not want key opinion blockers.
THE QUESTION EVERY FOUNDER SHOULD ASK
Liz: What is making you most excited about what you see happening in the broader space?
Alex: In the peripheral nerve space, there has been very little real progress for a long time. That is interesting.
The bigger question, what assumption could most be challenged right now, I think it is simply the assumption that neurological conditions just do not do well.
That is endemic. It is in the surgeons, the physicians, everyone.
We live in a world where neurological problems are, to some degree, the heart sink category. We do not know what we can achieve with them.
When industry comes in with something new, it hits that cynicism first.
We have a responsibility to bring things to market that make a difference. Not incremental improvements dressed up as something bigger. But as more change happens, as real ideas turn into real data and real outcomes, you start to create a mindset shift within the medical community.
And that generates genuine excitement.
Liz: And the medical world must change alongside the technology.
Alex: It must. But it is always slow. Medicine trusts anecdotal experience above almost everything else. Breaking years of ingrained thinking takes good quality research, real data, things that change practice and change patients’ lives.
That is why I think the question every company in this space should be asking KOLs early is not, here is our data, what do you think?
It is: what would I have to show you/ change in my solution to make you believe in this sufficiently to give it a go?
You learn more from that one question than from almost anything else.
CLOSING REFLECTIONS
I have thought about that question a lot since speaking with Alex.
It is a disarmingly simple thing to ask. And maybe not enough of us ask it. We assume the data will speak for itself. Alex has spent long enough standing on the other side of that conversation, as the surgeon being pitched to, to know that it does not always work that way.
What he is building at Newrotex is not just a device.
It is a potential solution, made in silk and clinical data and patience, to give the “heart sink” patients hope.
The current gold standard harms people to help them. It sacrifices a nerve in one place to attempt repair in another. It causes guaranteed damage to attempt uncertain recovery. And when the gap is large, it often does not even work.
Five patients already know there is another way.
One of them was told he might not walk again. He is walking.
Helen Hide-Wright sits on a trial steering committee, reviewing data, making sure the next person in her position does not have to make the same choice she did.
Alex is still in the operating theatre every week. He still sees the cases where medicine runs out of road. He knows exactly what is at stake if the funding does not come through, and exactly what becomes possible if it does.
The rose is already growing along the trellis.
The question now is whether the investment community sees what five patients in Panama already know.
Do You Want to Be Featured?
If you are a CEO or Co-Founder and would like to be featured within my Leader In The Neurotech Spotlight, please reach out to me.
Are you a VC, FO, KOL, researcher, or clinician with a specialist interest in Neurotech – then please also get in touch, as I want to have a well-rounded perspective.
Thank you.
Understanding The Brain-The Ultimate Frontier.

More to explore