
PROF. DR. BERNHARD MEYER, DIRECTOR OF NEUROSURGERY, TUM KLINIKUM – NEUROTECH KOL IN THE SPOTLIGHT
ABOUT LIZ MOYLES – HEAD OF NEUROTECH, CRUXX, AUTHOR

Liz Moyles is a self-described frustrated neurosurgeon. A lengthy hospital stay in her teenage years left her with PTSD and a fear of hospitals and blood, rerouting her career path entirely at 18.
Medicine was the plan. Biochemistry became the reality. But life in a lab was not where she belonged. What never left her was her fascination with the brain and the people building in the space.
Today, as Head of Neurotech at Cruxx, she works with start-ups and scale-ups across the US, Europe and beyond to help them attract the talent and capital required to build.
Her aim is simple: to give CEOs and leadership teams their time back to operate at a strategic level, not get pulled into day-to-day execution.
Fundraising, clinical trials, and regulatory work already stretch teams thin. Hiring sits on top of all of it.
When it goes wrong or moves too slowly, the consequences are immediate. It can mean missing funding, delaying submissions, slipping milestones, or losing people through overload.
Liz leads global executive searches for VCs and neurotech companies, placing C-suite and board-level leaders and building out senior teams across the US, Europe and beyond.
Embedded in the neurotech ecosystem, she speaks regularly with founders, operators, KOLs and investors, giving her a clear view of where the field is heading and what it takes to succeed in a start-up. That perspective shapes how she approaches hiring.
In start-ups, every hire matters, and attracting the best is non-negotiable. But they are rarely looking. Busy building elsewhere and often unaware of what you’re doing.
Finding them is one challenge. Getting them to engage is another.
But while you and your hiring managers are trying to find these people, the clock is running. FDA submissions, fundraising rounds, clinical trials.
Everything that cannot wait is …………waiting.
Reach out to Liz. That person is out there. She knows the space and where to find the people.
They just don’t know you exist. Yet!

A PEEK BEHIND THE CURTAIN
Some guests arrive with a polished narrative ready to go.
Prof. Dr. Bernhard Meyer is not one of those guests.
He is one of the most consequential figures in European brain-computer interface research today. Director of Neurosurgery at TUM Klinikum Rechts der Isar in Munich, where he has led his department for twenty years. More on what he has built later.
But first, the man behind the science.
Bernhard allowed me a rare glimpse, to go behind the curtain, to see who he really is.
And what I found was paradoxically complex and deeply likeable individual whose humanity makes everything he has achieved even more compelling.
He is intensely direct.
Self-confident to the point of putting some people on the back foot – me included, at times! But what I came to understand is that what Bernhard is really doing is pushing others to see and think differently.
To question the norms. Stretch their thinking. To question “what if?”
He will give you his honest opinion. If he disagrees with an idea, a concept, a direction, he will explain precisely why and very directly.
Not maliciously, but with a clarity that can hit hard.
He is, by his own admission, not universally liked. Always widely respected. His insights, knowledge and expertise unquestioned.
And yet he told me something I was not expecting to hear from this man.
Increasingly, the impact his delivery may have bothers him to a degree. He still stands by the substance of what he thinks. But today he is increasingly conscious of the way it lands. And he is now trying to change his delivery.
That he is even aware of the distinction – that he holds the internal conflict with honesty rather than defensiveness – and that he was vulnerable enough to share this with me – I found deeply human. I liked him even more for it.
And what of the KOL himself?
Many of us know him for his outstanding achievements as the Director of Neurosurgery at TUM Klinikum Rechts der Isar.
Here over 20 years he has built something that exists almost nowhere else on earth: a single institution where neurosurgery, neuroscience, and engineering work as one team, on real candidates, with real stakes.
In 2022, his team performed the world’s first BCI implantation in a candidate with post-stroke aphasia. A woman who has a language problem.
In 2025, his team became the first people in Europe to implant a BCI in a candidate with tetraplegia. It led to a 26-year-old man learning how to move a cursor with his thoughts.
Neither of those firsts happened by accident.
They happened because 12 years ago, on a morning bike ride to the hospital, Bernhard Meyer asked himself a question: “what could we do that will still stretch science ethically in 30 years from now?”
I sat down with him to find out the answer.
A BOLT OF LIGHTENING
Liz: Bernhard, take me back to the very beginning. Were you always headed toward neurosurgery? Was there a young Bernhard who dreamed of operating theatres?
Bernhard: No. I can’t say I was thinking about it from kindergarten,
But I always knew I’d be a surgeon. My father was a surgeon, and I thought it was a very meaningful way to work and to live. When I went to medical school, I thought I’d end up in general surgery, maybe orthopaedics.
It was only in my final year, when I did an elective in neurosurgery, that my direction changed, it was like a bolt of lightning. I was immediately transfixed,
I realised this was a field where you can do so much.
Glioblastomas in the brain, things that are so challenging and debilitating. Things we do not understand.
Liz: I love that insight. Tell me, were there people early on who really shaped you – not just as a surgeon, but as a thinker?
Bernhard: Yes, Two people.
My first manager was an outstanding surgeon. He looked like a huge bear. You’d never imagine someone of that size could do tiny, delicate things under a microscope so elegantly. He shaped me in terms of pure craftsmanship. The diligence. The patience. How you actually do it. In fact, bizarrely – he is turning 80 today!
My second mentor shaped how I think. About neurosurgery, about science, about what academic medicine is for. I spent 13 years with him.
He taught me that being a very good surgeon is the prerequisite, not the destination.
And he pushed me to think laterally.
He’d say: “I don’t want to read a paper about your 200-candidateand their splendid results. That’s not interesting. People already know it can be done. I want you to ask – “what is no-one else asking”.
Liz: That’s bizarre that we are speaking about your first mentor and it’s his birthday today! It sounds like their influence has never really left you.
At what point did you decide not general practice, but the academic route was your destination- and what does that this actually mean?
Bernhard: Quite early on.
The prerequisite of being in an academic environment is that you are a very good surgeon. That’s a given.
But you’re not there to fulfil routine surgery brilliantly.
What you need to do is push the limits of your field so that what was is very difficult today can be routine in 20 years from now.
When I began, the medical world believed 65 years old was the upper limit for operating on a candidate with a malignant brain tumour.
Nowadays, octogenarians are roughly 40% of my patients. You’re walking a thin red line.
Push too much and you put patients at harm. Don’t push and there’s a cost in the other direction too.
And it takes enormous effort to move forward by a tiny step in clinical progress.
Initially that’s very frustrating. But you learn gradually that even though the progress you are making appear painstakingly slow, when you look back a year or two, the progress is substantial.
All because you kept deliberately taking those very tiny steps towards your destination.
Liz: That’s a great way to look at it and probably something we could all benefit from doing Bernhard. Earlier, you mentioned glioblastoma patients. How do you approach patients who are in such dire circumstances?
Bernhard: Most candidates come to me after they learn their average life expectancy is very short.
I’m a very busy surgeon and I don’t talk about things that aren’t important, but I do take time with these patients.
The first thing I tell them is “get rid of this idea of the average”.
They need a different perspective.
I tell them: “you’ll belong to the 70% still alive after two years. You’ll belong to the 40% still alive after five years. And who knows what happens in those five years?” Just because I can’t cure a candidate today doesn’t mean something won’t happen to change that in the next 5 years.”
I don’t tell these individuals “There’s nothing we can do for you.”
The opposite is true. And if you look back over the last 15 years, the percentage of glioblastoma patients surviving 2 or 5 years has increased dramatically.
Because those tiny steps. They add up.

A MORNING BIKE RIDE
Liz: I can imagine that it’s a life changing moment for them. Please tell me about the culture inside your department.
Bernhard: Every morning I either jog or cycle to the hospital. And in those 30 minutes, I think about what I might do differently, that day. What I might add.
Then after the morning conference, I talk to my team. I throw in ideas and I wait to the next day to see what they come back with. I’ve done that for 20 years.
Liz: What are you actually testing when you do that – the idea, or the person?
Bernhard: Both. I want to know who can think laterally and who can’t. Who is satisfied that what they’ve achieved is working and doesn’t want to change anything – the “never-change-the-running-system type”.
And who amongst them is restless and doesn’t want to stand still. Obviously, I prefer the latter.
But I accept we need the others too, because I can’t change people’s personalities.
And the truth sometimes lies in the middle. Very often my final decision is affected by the input I get from people who aren’t like me at all.
Liz: And what does the less restless person actually contribute in your team?
Bernhard: I need the dedicated clinician who does routine at an exceptional level and whom I can completely depend on. That is their value.
What I require in return is loyalty, and an acknowledgement that their time in this department is limited, because I only take people into my team who have an academic focus.
I have a mentorship programme. Every year in February and March we evaluate all the trainees, give feedback, and from the start I tell them honestly: you’re going in this direction, or that one. And I tell them very frankly that if research isn’t in them, if they don’t feel it, then they should just tell me.
I’m fine with it. I just need them to be exceptional clinicians. Then their time here ends, and they move on to a fellowship or whatever. Everyone knows from the beginning that is the way things go.
My oldest attending is 38 years old. 50% are female. Things have evolved. Once people reach staff surgeon level, I’m on first-name terms with them, despite the fact they could be my children. It’s more like a family. You have to be on the inside to see what’s really going on.

Liz: Let’s talk about when the BCI focus began for you.
Bernhard: It was about 12 years ago.
I was thinking on one of those morning bike rides- what could I add to my portfolio? What would be interesting in 20, 30, 40 years.
And it was partly by chance. I thought, of BCI and why not?
I had a friend working in Los Angeles doing related things. I called him. He said he was having the same thoughts. And that’s how it started and if I do something, I do it right.
The preparation for my first procedure took at least 12 years.
To be honest, at that time I didn’t even appreciate what I was taking on and the implications. I couldn’t have foreseen what has happened now.
Part of it is luck. I found it and it found me at the right time.
Now I’m thinking- “what next? What do I want to achieve in the next 5 years. What do I want to leave behind? What is something the department can build on after I’m gone.”
Initially, the BCI field was considered cynically. “That’s never going to work. And if it works, it’s never going to develop.”
But then along came artificial intelligence. The development of machines, how they work. 20 years ago, you implanted something, but you couldn’t do anything with the signal. It took ages to understand even a simple tiny movement.
Now it’s all happening in an exponential fashion. And the next 5 years will be decisive.
We’ll see who is in the leagues, academically and surgically, and who is just going to tag along.

Liz: You were the first surgeon in Europe to implant a BCI in a candidate with tetraplegia. The young man from the motorbike accident. But that wasn’t your first chronic implantation, was it?
Bernhard: No. Our first chronic implantation was 3 years before that.
A woman who developed aphasia after a stroke.
Not just a speech problem- a language problem. Those are two different things.
And our first acute implantations took place 8 years ago. So, we go back further than most people realise.
The decision to start with the aphasia candidate rather than the motor deficit was mine.
Nobody else had done it.
At that time there had been 30 or 40 implantations for motor deficits worldwide, and I thought: “that’s not so innovative. It is not so unique. We can do motor deficit later.”
And that’s what happened. We were very quiet about telling the world. We didn’t go public because it was unknown territory. We didn’t know what we’d do.

Liz: Tell me more about the lady with aphasia.
Bernhard: What we found was extraordinary.
That piece of research is funded by the European Research Council. Over 10 months we examined more than 10,000 neurons in the intact right hemisphere of her brain while she performed language tasks.
The undamaged right hemisphere actively takes over language functions after the dominant left hemisphere is damaged. Individual neurons respond specifically to words, their meaning, their phonological structure. The neural code remains stable for many months. We began to identify which word she was trying to say from her signals alone.
We published our preprint on this recently – the world’s first study examining how individual neurons in the right hemisphere process language when the left is damaged.
We were able to show that the human brain remains adaptable even after severe damage – even if aphasia has been present for years. That is truly exciting and opens entirely new possibilities for rehabilitation.
Liz: That research has attracted serious attention. The Frankfurter Allgemeine Sonntagszeitung gave it a double page spread in their science section. The NZZ dedicated an entire podcast to your work – they called it Quantum Leap. That kind of coverage says something about how significant this is being seen to be.
Bernhard: Yes. And with that comes responsibility.
We’re a publicly funded academic institution, supported by the German Federal Ministry of Research. Scientific leadership, clinical responsibility, transparency, ethical guardrails – these aren’t optional for us. They’re the foundation.
The work has also brought politicians into the lab. We recently hosted several German parliamentarians at our Laboratory for Translational Neurotechnology. The question at the centre of that conversation is: “how can neuroscientific research from Bavaria help people worldwide, and what framework conditions are needed to advance innovation responsibly?”

Liz: I’d like to go into the ethics with you shortly if we may. But please can you tell me about the first motor deficit operation in 2025?
Bernhard: Yes. It was done with Michael Mehringer who is 26 years old.
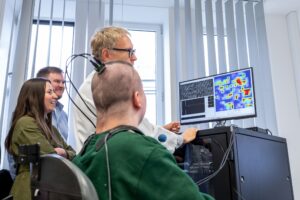
Paralysed in a motorbike accident. He still has a plug in the back of his head – we’re wired, not wireless yet. He comes to the hospital twice a week.
He can already control a cursor on a screen using only his thoughts. A robotic arm is next.
Michael was the ideal candidate. Not because we felt sorry for him, but because of who he is.
He’s so positive. He knows that when he goes back to his village, he’s a hero. He knows his name will be remembered longer than mine, probably, in 30 or forty years from now. And righteously so.
I’m fine with that. Today, worldwide, about 100 people have a brain implant. Most of them are in the United States.
Michael is the first in Europe with this indication. That matters.
Liz: Bernhard, I notice you never say patient. You refer to candidates. Why is that?
Bernhard: Yes. They’re not really patients. They’re members of the group. They’re part of the experiment.
People – and the candidates themselves – need to realise that their own personal benefit will probably be limited. They will benefit, but the benefit for the community, for humanity, is incomparably larger. What they’re doing is deeply altruistic.
That’s the first thing an ideal candidate needs: despite their situation, an altruism that is higher than average.
But on the other hand – every human is vain.
The last candidate we implanted, Michael has found a new purpose.
So, there are actually two opposing characteristics you need. Altruism. And a certain healthy selfishness. Both.

Liz: And attitude? Does it matter whether a candidate is fundamentally a positive person?
Bernhard: Highly important. This man thought he was going to live forever, even before the implantation.
And even more so afterwards.
If someone wakes up every morning fearing what their restrictions mean, contemplating what the future looks like – they are not an ideal candidate.
You need to work with people who say: “this happened to me. It sucks. But I am coping. I can cope. I’m normal, even though I can’t move a finger or express a thought. I’m going live as normal a life as I can.”
They also need an intact social environment. Family support. Without that, it doesn’t work.
The process of finding the ideal candidate takes a long time. We now have enough experience to know very quickly whom not to consider. These are candidates. They’re not patients.
They won’t benefit in the way they think. In the press, it’s always portrayed as this team are helping the patient. We do help. But not primarily the one we implanted.
Liz: These individuals need to trust you profoundly. How do you handle this?
Bernhard: The neurophysiologist who heads our translational neurotechnology lab is Simon Jacob – the scientific architect of this programme. He and I are opposing personalities.
He’s not dangerous, in the eyes of the candidates. They always ask about whether we will be reading their brains, their thoughts.
Simon is wonderful. He is just brilliant at handling all these and other concerns, earning their trust, ensuring they know we will never exploit them.
But trusting me is harder initially, because I’m the one who will hurt them again. I’m the one who is going to open them up.
So initially I stay in the background. Out of sight, out of mind. They have enough to process before coming face to face with me.
And then, the moment eventually arrives when they are ready and need to meet the one who will actually do it.
Without Simon, none of this exists.
Once we’ve selected a candidate, the mapping begins. We meet regularly. They get to know us. We get to know them. You need time to earn that trust. And you can’t rush it.
CROSSING THE LINE – SUPERHUMANS
Liz: How hard was it to get the Ethics Board on side in the beginning?
Bernhard: It took about a year to convince them initially.
Obviously, they wanted to understand and test the concept from every angle. What are they doing? Why are they doing it?
But now the process to a decision takes a week and soon we’ll be implanting other patients. Because they trust what we do and they see the results. They’re smart people. They know it’s better to have one of us doing this. Better us than many other people in the media I could name.
Our Ethics Review Board is a core member of our group now. Whenever we plan something new, they’re in the room from the beginning.
Liz: When you look at where BCI is heading over the next five years, what do you think most people are missing?
Bernhard: 20 years ago, you implanted something and couldn’t do anything with the signal. It took ages to understand even a simple tiny movement. Now it’s all happening in an exponential fashion. As I said, artificial intelligence changed everything. And the next 5 years will be decisive.
Liz: And where does TUM sit in that race, honestly?
Bernhard: We’ve conducted the world’s largest series of microelectrode measurements in the human brain.
We’re the first academic institution in Europe to have implanted 2 BCIs.
The combination of medicine, neuroscience, and engineering under one roof – there are very few universities in the world that have all three core disciplines at a single site the way we do.
Publicly funded. Ethically anchored.
That’s a different position to the commercial players.
But I’m also honest about the competition. @Neuralink is already further ahead on wireless capability.
Their devices don’t require a physical connection. Ours still do – Michael still has his plug. That’s the next engineering challenge.
The train has left the station. If you want to shape the future of BCIs, be a steadying force, whether you agree with it or not, you can’t observe. That is hopeless.
If you want to influence, you must be in the race and you must lead.

IT’S UNSTOPPABLE
Liz: Whilst we are talking about ethics Bernhard, there’s talk of creating super -humans, enhancing healthy individuals cognitively. Where is the line, and who gets to draw it?
Bernhard: The question is: at what point do you cross from treating a candidate with an illness, to enhancing a person who simply has a weakness – maybe a difficulty calculating, a problem with memory that falls within a normal standard deviation?
Because once you consider enhancing those people, you’re crossing a line that is very debatable.
And since I’m a doctor, I could say: well, it’s that’s not my problem. I’m just helping candidates.
But the truth is: by introducing this technology, I am someone who has opened the gates. I can’t simply close my eyes and say ’that’s not my problem. Someone else can deal with that.
Part of me created it this situation. So, it is my problem.
And I want to influence the future. I have a voice and an opinion, and I will use that to try and ensure that lines are not crossed.
Take plastic surgery. You have the two poles. At one end: someone who has been scarred in a fire, a mastectomy. Plastic surgery for them is entirely beneficial. Nobody debates it.
At the other end: a 17-year-old choosing cosmetic surgery because of how she looks. That is also plastic surgery.
Gradually there’s been a transition in society from what society accepts to what it doesn’t and the lines have been blurred there. Will this happen with the brain? Probably. That’s the reality. Over time, the lines will blur.
The question will be debated -is it an illness if you cannot calculate? Or just a personality trait?
Sooner or later, someone will cross that line. Either a capitalist with no limits, or a state with no limits.
Liz: And you think it’s unstoppable?
Bernhard: Yes. Everything that’s possible today has been done by humans.
Why would this be any different?
Look at ChatGPT. When it launched, politicians tried to ban it for a year. Impossible to stop.
Two or three years later, everyone uses it: privately, professionally, in every field. No one questions it. People use it for recipes and everyday tasks it’s that accepted. It isn’t even questioned or commented on.
That’s why I say you have to be on top of it.
If you are part of the discussion rather than a disapproving bystander, you control the development, and you’re at least capable of shaping what happens.
If you avoid the discussion, ultimately it will hit you. And you’ll have no weapons.
Investors like Musk aren’t in this purely to help people. Even if they help many. I don’t believe that’s the only reason. They know the real money will come from crossing that line.
Once you cross the line we just talked about, once you’re talking about essentially everyone having a biological and electronic brain, then this will be very big business.
That’s what motivates them. They openly talk about this.
And then there’s the other motivator. War is the father of all ideas – from ancient Greek onwards. That’s still true, more than ever.
If you want to win in the future, you must think decades ahead. The investments being made in defence and state-level capability around neurotech is phenomenal.
They are some of the biggest investors- why do you think they are doing it? To help their injured soldiers or in the case of states – their populations?
Bernhard: Why do you think it is frightening Liz?
Liz: Well for me for example, there’s talk of living forever. I don’t want to live forever. This has been eventful enough, thank you. I don’t want to communicate telepathically. And then there’s all the other potential situations I can’t even imagine, but that will exist.
Berhard: But they may become the norm. Unquestioned. Unchallenged. Like ChatGPT Liz.

TINY WHEEL. FIRM FOUNDATION.
Liz: So true Berhard and it is frightening in some respects. I’ve done my homework on you Berhard. You haven’t mentioned the Lifetime Achievement. Come on tell me about that!
Bernhard: Ha ha. Yes, at the end of last year at the EANS Congress 2025 in Vienna I was honoured with the EANS Lifetime Achievement Award.
It is a great honour for the TUM University Hospital. The award was presented by Congress President Professor Claudius Thomé at the Congress of the European Association of Neurosurgical Societies (EANS) in Vienna.
Liz: Ok. I’m going to read out what the clip says as I don’t think I’m going to get much more out of you.
The award was presented “In recognition of Meyer’s “outstanding contributions to the field of neurosurgery, especially in spinal research.”
And it says you said – “This prize is a great honour for me, a recognition of my efforts over the past three decades,” said Prof. Meyer, thanking the EANS . The neurosurgeon initially focused his research on epilepsy and congenital vascular malformations in the brain and spinal cord before turning his attention to the spine. “Because I realized that one has to concentrate on diseases that are more common, in order to offer even more individuals, the best possible therapy.”
In Germany alone, many millions of people suffer from back problems, some of whom require surgery. This often applies to people with spinal injuries as well.
Those affected also benefit from Meyer’s efforts to promote collaboration between medical specialties, such as trauma surgery-initially despite considerable resistance. This initially bumpy road has proven worthwhile:
“You have to leave your comfort zone,” says Meyer. “If you stay within your own community and don’t open yourself to the expertise of others, you’ll never make progress.” And: “I think this was a major step for neurosurgery: Now we are leaders in this field– and I’m truly proud of that!”
Liz: Wow Berhard. That is simply phenomenal. This may sound a stupid question given the above, but I know for many awards are nice but it’s not what they strive for. When you finally walk out of that department, whenever that day comes, what do you want to have left behind?
Bernhard: When I leave, I want to be out of here.
I don’t want to still have an office here.
There’s nothing worse than the grumpy old man who stays on in a small office and pesters his successor.
My successor should be better than me, building on the foundation of what we’ve built.
I’m vain. But not that vain!
In terms of legacy- I’m not thinking at the scale of an impact on mankind.
I’m a tiny wheel in a very large machine, and I’m aware of that. Progress takes tiny steps and enormous effort. I’m fine with that.
What I want to leave is something others can build on. Something where people say: that was innovative. It helped to move the field forward.
Nothing more than that.

Liz: Berhard I know that people already think and know that what you have already achieved has done that. My hope for you would be that the people who follow you speak about you the way you spoke about your two mentors today.
At this point Bernhard chuckled and looked quite emotional and almost nostalgic. It was a very poignant moment.
Berhard: That’s one thing I hope too. I can already see some of it. I have around 10 people who’ve gone on to take Chairs, who came from me. And basically, everyone thinks very positively. That’s important. That’s good.
Liz: How do you deal with the tension between what you’re doing and the more conservative end of the neurosurgical community – the surgeons who are resistant to a particular change?
Bernhard: Once I consider something that was innovative for me and my team as now routine, my job is to convince other people it is routine.
And if I can reach that – if I can get them to exchange what they were doing before for this – I’m happy.
I don’t expect people to immediately say yes and change.
If I propose something counterintuitive, the normal reaction is: what is he doing? That’s fine. But if I have convincing arguments, and if it’s proven in environments outside my own service, then I expect someone to at least consider it as part of their practice.
Liz: And how long does the journey from academic research to real clinical adoption actually take?
Bernhard: It’s a very long and frustrating thing. Often 10 years. You need patience. Real gamechangers are very, very rare. Otherwise, they wouldn’t be game changers.
Liz: From our conversation, I know there’s something you’ve been reflecting on more recently. Something quite personal. I found it one of the most honest things you said to me.
Bernhard: I’ve always been direct with my opinions. Never malicious. Just factual and reasoned. If I disagree, I say so and I explain why.
I know that people respect me even if they don’t like what I say. And some don’t like me for it. It doesn’t make me popular or universally liked. I know.
Until very recently, what other people thought of me didn’t bother me. But for the last few years, it has begun to somewhat. Not to an extent that I doubt what I do or think.
But how I deliver my thoughts and opinions is now something I am considering more.
My wife is also a neuroscientist. She’s probably the one who criticises me the most. My children know all my weaknesses. We’re very open at home – to the extent of being painful sometimes.
If people think I am a certain way, then for them, that is reality. You can’t argue with that. You must learn from it. The development of your personality ends when you go to your grave. Not before.
Liz: That takes real courage to say out loud. Thank you for trusting me with it.
Bernhard: At least I’m aware of it. That’s probably the most any of us can honestly say.
A CLOSING THOUGHT FROM LIZ
I have thought about this conversation a great deal since we spoke.
Bernhard Meyer is one of the most formidable people I have interviewed in this series. His insights are very interesting and his directness unique. He is also one of the most unexpectedly human people I have interviewed.
He runs one of the most significant BCI research programmes in the world.
He has performed procedures no one else has performed. He leads a department that has produced science that will outlast all of us.
He sits with glioblastoma candidates and tells them to throw away the average.
He cycles to work every morning asking what he might do differently. He chose aphasia when everyone else chose motor. He invited politicians into his lab. He told the NZZ that the next 5 years will decide everything – and then went back to the hospital to keep building.
Very few people live daily asking what will still matter in 30 years from today.
Most of us are managing what already exists.
Bernhard seems inherently programmed to be different – not recklessly.
He is, if anything, unusually rigorous about ethics, consensus, and accountability.
When he leaves TUM he won’t be the grumpy professor in the side office overseeing his successor. He’ll walk out forever.
I know there will be many who have trained under him who will regard him as the mentor that most changed this thinking and that he will achieve this legacy. He probably has already achieved that.
But until then, the morning bike rides will continue, and Bernhard will continue asking “what am I going to do differently today?”
Do You Want to Be Featured?
If you are a CEO or Co-Founder and would like to be featured within my Leader In The Neurotech Spotlight, please reach out to me.
Are you a VC, FO, KOL, researcher, or clinician with a specialist interest in Neurotech – then please also get in touch, as I want to have a well-rounded perspective.
Thank you.
Understanding The Brain-The Ultimate Frontier.
More to explore
