Leader in the Neurotech Spotlight: Prof. Dr. Vitor Mendes Pereira
ABOUT LIZ MOYLES – HEAD OF NEUROTECH, CRUXX, AUTHOR

Liz Moyles is a self-described frustrated neurosurgeon. A lengthy hospital stay in her teenage years left her with PTSD and a fear of hospitals and blood, rerouting her career path entirely at 18.
Medicine was the plan. Biochemistry became the reality. But life in a lab was not where she belonged. What never left her was her fascination with the brain and the people building in the space.
Today, as Head of Neurotech at Cruxx, she works with start-ups and scale-ups across the US, Europe and beyond to help them attract the talent and capital required to build.
Her aim is simple: to give CEOs and leadership teams their time back to operate at a strategic level, not get pulled into day-to-day execution.
Fundraising, clinical trials, and regulatory work already stretch teams thin. Hiring sits on top of all of it.
When it goes wrong or moves too slowly, the consequences are immediate. It can mean missing funding, delaying submissions, slipping milestones, or losing people through overload.
Liz leads global executive searches for VCs and neurotech companies, placing C-suite and board-level leaders and building out senior teams across the US, Europe and beyond.
Embedded in the neurotech ecosystem, she speaks regularly with founders, operators, KOLs and investors, giving her a clear view of where the field is heading and what it takes to succeed in a start-up. That perspective shapes how she approaches hiring.
In start-ups, every hire matters, and attracting the best is non-negotiable. But they are rarely looking. Busy building elsewhere and often unaware of what you’re doing.
Finding them is one challenge. Getting them to engage is another.
But while you and your hiring managers are trying to find these people, the clock is running. FDA submissions, fundraising rounds, clinical trials.
Everything that cannot wait is …………waiting.
Reach out to Liz. That person is out there. She knows the space and where to find the people.
They just don’t know you exist. Yet!

I caught Prof Dr. Vitor Pereira on a Tuesday morning in between cases.
He had already done two surgeries that morning. Two more were coming that afternoon.
We planned a 40-minute call and spoke for 90 minutes. The time flew, and I felt we had barely scratched the surface.
Vitor is a multi-layered individual. Confident and humble. Excitable, passionate, funny, driven. He thrives in the face of unsolved problems.
After we spoke, he would go on to perform a couple more surgeries that afternoon.
He had also led a foundation funding meeting, spent time spent helping a junior colleague through a complex procedure, run a session with his fellows, a research review, and was planning the next phase of Project Robo Angel, the remote robotic stroke programme he will be expanding globally.
This was another routine Tuesday but also a great Tuesday as he told me.
He needs little introduction.
Prof. Dr. Vitor Mendes Pereira is Director of Endovascular Research and Innovation at St Michael’s Hospital in Toronto, Professor of Surgery and Medical Imaging at the University of Toronto, holder of the Schroeder Chair in Advanced Neurovascular Interventions, and Lead Scientist of the RADIS Lab.
He has contributed over 270 publications to his field. He has accumulated more than 46,000 citations.
He is by his own admission probably one of the busiest neurosurgeons of his specialty in Canada.
He has also spent 20 years performing procedures that did not exist before he performed them.
But none of that is where the story starts.
The story of Vitor starts on a farm in north-east Brazil. A boy who wanted to build things. A father who left this world too soon and a young girl Andrea, who became the love of his life.
THE BEST KIND OF TUESDAY
Liz: Hello Vitor, and thanks for making the time to speak to me. What has been happening for you today?
Vitor: Hi Liz. Lovely to speak again. Everything is going well. Surgery is going well. I’m in between cases. I’ve completed 2 surgeries this morning and have 2 more this afternoon.
I’ve had a few successful meetings already and we are aligning some great projects. My team are happy and that makes me happy.
Earlier, I helped a junior colleague work through a complex procedure I want him to be able to do on his own one day.
I also helped my Fellows with a case. I had a meeting with our Foundation about future funding for the research programme.
And this afternoon I am going to review our research projects, including the continuation of Project Robo Angel. That is the remote robotic programme we just launched in Panama. We are expanding it globally now.
This is a great day Liz – a big day and a good day for me.
Liz: Vitor, how on earth do you balance all this with the research work what motivates you because you clearly love what you’re doing?
Vitor: I do 4 days of clinical work a week. Surgeries, consultations, stroke and brain aneurysm call. I love my clinical practice. I love the consultation with patients. I love to help.
It makes me feel alive, happy, satisfied.
There’s little better than walking in to see a patient after surgery and being able to tell them that their surgery has been a success, and to watch them go home, smiling with their families!
I get joy from seeing one of my Fellows presenting at a conference, learning that a student I once worked with has become someone important in the field, getting a research paper published.
Those moments fulfil me enormously.
The other thing that motivates me is the unsolved. I carry cases. Complex cases that I have thought about for years.
Situations I could not solve the way I wanted to. They stay with me.
I keep thinking, how could I have done better? How can I help the next time?
Those unsolved problems are honestly where most of my research ideas come from. The problems I cannot let go of, become the cases I go out and try to solve.
THE ISLAND, THE FARM, THE FATHER
Liz: It’s fascinating and your energy is palpable. I’m getting excited listening to you. But tell me, Vitor, did you always grow up wanting to be a surgeon?
Vitor: No, nothing could have been further from my mind!
I grew up on an island in the north-east of Brazil called Sao Luis do Maranhao. It sits between the city and the countryside.
My father was a federal highway patrolman, and my mother was a public health nurse. So from the very beginning, discipline, public service, education, were the central values in our home.
As a kid I was completely fascinated by technology. I wanted to be an engineer- I loved that and technology and computing. That was the plan.
Then in my last year of high school, two things happened that changed everything. I started dating Andrea, the love of my life. And my father was diagnosed with prostate cancer.
I put my career plans on hold. I helped take care of him. I helped run the family farm. I stayed close to Andrea and close to my father through everything that came after that.
Supporting him through his illness made me realise something I have never been able to let go of. If he had been managed appropriately, he likely would have survived.
The information that should have been there was not there when it needed to be. That left me feeling completely helpless.
So I decided to change my direction. I didn’t want this to happen to any other families. I decided I was going to pursue medicine. My interest in engineering and computing did not disappear. It just redirected. Understanding medicine became a way of helping others.
The Brain. From the First Patient.
Liz: And once you were in medicine, what made you focus in on the brain?
Vitor: During medical school at the Federal University of Maranhao I started shadowing a neurosurgeon named Periguari Lucena. And I knew from the very first patient I helped treat, that neurosurgery was what I was going to do. It was just clear to me.
I became fascinated -the precision of neurological examinations. The complexity of it. Nothing else came close for me.
During my residency at Sao Paulo State University, a vascular neurologist named Cesar Raffin turned my attention to stroke patients.
My preceptor Marco Zanini taught me everything about brain aneurysms. And then I did rotations in neurointervention under Guilherme Caldas and his team. I learned angiography. I learned the principles of endovascular intervention.
And I fell in love with it completely. The brain, through the vessels, minimally invasive. That was the direction I wanted to go.
But I also knew that the best place in the world to train in this specialty was Paris. And I knew that getting there was going to be very difficult. You needed references. You needed to work through many people. It took years just to be considered.
I was determined to go and study there. So, I found a way in.
I READ EVERY PAPER. FROM THE 1800s ONWARDS.
Liz: How did you achieve that then because that’s not an easy school to enter?
Vitor: During my residency I took no vacation for 2 years. I saved every single day I was owed. I accumulated 2 months leave, and I used all of it for an Observership in Paris with Professor Pierre Lasjaunias, one of the great figures in our field.
While I was there, we encountered a very rare case. A patient with neurofibromatosis and a fistula in the neck. Professor Lasjaunias asked me to study it. To really study it.
So, I read everything ever published on neurofibromatosis. From the 1800s to 2005. Everything.
At the end of the Observership I gave a presentation on the work I had done. What I did not know was that the room contained the biggest specialists on neurofibromatosis in Paris. I had no idea. I just presented what I had found and answered every question they asked me.
Afterwards Professor Lasjaunias came to me. He asked me: “do you have any idea who was in the room listening to you just now? do you realise how confident you were?”
I asked: “No Professor. Who are they? I don’t know if I sounded confident but you asked me to study neurofibromatosis so I just read everything I could find on it.”
He said: “everything?”
I said: “yes.”
He then effectively changed my world and he said to me: “I suggest you do your master’s thesis on it.
And I asked him, “Can I come and be your Fellow?”
He said: “obviously. You can start tomorrow!”
I had to go back to Brazil first to finish my residency. He held the position open for me.
“Your place here is guaranteed”- he told me. And the following year I came back.
Liz: Wow. That feel like fate and a lot of hard work. There is so much to learn in that story. You worked really hard to make something that would probably have been impossible, become reality. Even getting to work with both Lasjaunias and Moret- 2 of the absolute biggest names in your field.
Vitor: I was very fortunate. God smiled on me.
When I was with Professor Lasjaunias, there were some surgical techniques he did not personally offer which I wanted to learn. I wanted to know everything.
He suggested that if I wanted to learn those techniques, the best person to go to work with would be Professor Jacques Moret at the Rothschild Foundation.
A friend also warned me that it would be very difficult to get a place there, especially at short notice. Before I could actually start to plan out how I would make this happen Professor Lasjaunias picked up the phone.
In front of me. He called Professor Moret himself. And Professor Moret gave me a place!
I arrived at the Rothschild Foundation as Professor Lasjaunias’s protege. The team there was extraordinary. Charbel Mounayer, Laurent Spelle, Michel Piotin, Raphael Blanc. I shaped my practice working alongside those amazing mentors and people. I made friends for life.
And then while I was there, my world turned upside down. Professor Lasjaunias, my great friend and mentor died. I still miss him today. He was a wonderful human being.
Professor Moret didn’t hesitate. He came to me and said: “I will take care of you.”
And he did. He adopted me professionally. He became my second great mentor. I am still astonished, to this day, that I was trusted by both of those men.
I am truly blessed to have been mentored by 2 of the people who transformed our field.
And whilst all this was happening, I had started a second master’s degree in Geneva and was doing weekend calls at the University Hospital there. I was trying to build in every direction at once and learn as much as I could do.
I was like a sponge.
They Offered Him the Department. He Built Something From Nothing.
Liz: So what happened in Geneva?
Vitor: It was incredible but the entire neurointervention team resigned and the hospital asked me to stay and cover for a few months.
A few weeks in, they offered me a permanent position. Then I became the Head of the Neurointervention in a few months, and they told me I could build my own service.
Liz: What? That is just incredible. Sounds like fate again.
Vitor: It was just unbelievable! These things just don’t happen.
The welcome package they extended to me included renewing all the technology, building a research team, effectively building a lab from scratch.
So, I recruited my own team. We invested in stroke treatment, in complex brain aneurysm treatment, and we built Geneva into one of the biggest stroke treatment hubs in Switzerland and in Europe at that time.
And that was where the innovation laboratory began. I started working on emerging technologies applied to neurosurgery.
I could see a movement coming and I wanted to be building it rather than watching it arrive. I wanted to be shaping it.
Then Toronto came calling. We talked for 2 years before I made the move.
Eventually I said yes. I have been in Canada for 12 years now.

UNETHICAL. IRRESPONSIBLE. THE STANDARD OF CARE.
Liz: And you’re obviously extremely happy here, but tell me, Vitor, what does it take to become a KOL?
Vitor: Yes, a strange term. I have always had a very scientific mindset. From the beginning my research started with Computational Fluid Dynamics and Biophysics.
From early on I got involved in device development. Advising companies. Testing prototypes. Giving the surgeon’s perspective to teams who are ultimately trying to make our job easier and our patients safer.
When I was in Geneva, I had the opportunity to be one of the first physicians in the world to work with stent retrievers for stroke treatment.
And I also built, over many years, what was then the world’s largest flow diversion experience.
Switzerland had a faster regulatory approval pathway for new devices than most other countries at the time. That gave me access to both technologies earlier than almost anywhere else.
Technically, Professor Moret had already prepared me to use them at the highest level. I published the first papers on flow diversion for complex and ruptured aneurysms from that foundation.
I was very early with the 2 techniques that went on to revolutionise our field.
I became a Principal Investigator on the early studies including the STAR study, the first prospective study with stent retrievers for stroke treatment and also on a randomised trial that validated stroke treatment in 2015, SWIFTPRIME trial.
And separately, I had trained the Dutch cohort of physicians in the new stroke techniques.
They went on to develop the MR CLEAN trial, (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke) in the Netherlands.
It was the first randomised trial to demonstrate the clinical effectiveness of endovascular treatment for acute ischemic stroke.
It was a Netherlands-based trial led by investigators at Erasmus MC in Rotterdam and Amsterdam UMC, and it changed the global standard of care for stroke treatment.
In parallel I kept pushing my own range. As I said I was steeped in computational fluid dynamics and biophysics but I also work across genetics, molecular biology, robotics and AI.
People sometimes ask how that breadth is possible. The answer is I never stopped being curious. I am just so curious. I love to learn, to as, to read.
I want to be more. I am a clinician and a scientist.
Liz: How did people react/ how do some people react to you questioning the status quo? Is it always welcome, or are you sometimes met with controversy?
Vitor: that’s a good question, Liz.
I had a lot of stones thrown at me and my team. People called me “a neurosurgeon doing experimental surgery on patients”.
“Unethical. Irresponsible. Experimenting.”
I’ve been labelled them all. Countless comments on social media. In conferences. I understand it. I really do. Change is uncomfortable. As surgeons, we always have to protect what’s best for patients. Lives hang in the balance.
You don’t experiment unless there’s a reason.
And yet all those techniques for which I was vilified, are now the standard of care and the best in class.
When I look around me, I see 2 types of physician. The fixed mindset and the open mindset.
– Fixed mindset physicians follow guidelines. They are safe. They will not deviate. But they will never evolve the field. They will never change the guidelines. And there will always be patients they cannot help, because new approaches take years to make it into a guideline.
– The open-minded physicians? They are the ones who change the guidelines. People like @Adnan Siddiqui. People who drive the studies. People who drive the innovation and then back it up with science.
And that is what I learned from my early stroke work and the criticism that went with it. The only way to face the people who resist, is to be completely backed up by research.
Every new idea you see from me, I have been working on it and publishing for at least 2, 3 sometimes 6 years before I go public.
The science comes before the claim.
Always. And I am now involved in writing the guidelines themselves, for robotics, for telesurgery, for neurointervention.
Because that is the only way to eventually bring the fixed mindset colleagues with you.

The RADIS Lab: Where the Ideas Go to Become Real
Liz: I hear that so much- science before the claim every time, is a strong way to move people towards change. Vitor, I’d like to move on now and talk about RADIS. What is Radis?
Vitor: It stands for Robotics, Artificial Intelligence, Dynamic Flow, Advanced Imaging, and Simulation.
The RADIS Lab was born from the convergence of clinical practice, engineering, and applied science. It is a translational lab. We take the latest technological and scientific innovations and we apply them to treat vascular diseases of the brain.
A key strength is the close relationship between clinicians and scientists.
My co-lead is Nicole Cancelliere, a radiation technologist with a master’s in neurosciences, and she has been with me from the very beginning.
She was part of the clinical team for the world’s first robotic neurovascular intervention I performed in 2019.
She has been and is integral to every step of Operation Robo Angel. And she has been an extraordinary partner in building everything the RADIS Lab has become.
We now have 12 researchers, and they all carry the same passion and the same mission-driven purpose.
I throw the ideas. We meet, we structure, we develop the protocols together. 20 years ago it was just me thinking alone. Now it is a whole team.
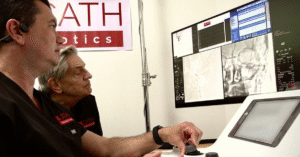
As I said, the world’s first robotic neurointervention was in 2019.
I had been chasing Mark Toland, then CEO of Corindus Vascular Robotics, for years to let me work on developing neurointervention with his system. He gave me a beautiful vase to celebrate that first procedure. It still sits on my desk. It means a lot to me!
Then the world’s first intravascular high-frequency OCT imaging in the brain.
This was a worldwide collaborative effort with Gentuity, the Massachusetts imaging company that makes the Vis-M probe, the University of Massachusetts where Professor Matt Gounis and his team led the preclinical work, and centres in Buenos Aires with Pedro Lylyk and beyond.
I performed the first human procedures here at St Michael’s Hospital, Toronto. The Vis-M gives us 10x the resolution of anything that existed before. Seeing inside cerebral vessels at micron level during a live procedure.
Direct visualisation of pathology and device interaction in the brain in real time. That changes everything about how we understand and treat these diseases.
And then now Operation Robo Angel with XCath and Eduardo Fonseca. Which is where we are now taking all of this past learning and experience.
200 Kilometres Away. One Patient. One Chance.
Liz: We have you mentioned Operation Robo Angel several times. Let’s talk about it in a bit further depth. What can you tell me about it?
Vitor: At RADIS lab, we have been working on remote connectivity for years, the safety parameters, the bioethics frameworks for telesurgery in neurointervention.
We have been meticulously building the scientific foundation properly so that when we performed our first telerobotic operation, it was done correctly.
With Eduardo Fonseca and Nicholas Drysdale at XCath Robotics, using their Iris Surgical Robotic System we made this possible.
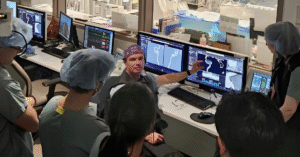
For one week, teams of physicians and clinical research coordinators staffed the emergency departments of 3 major hospitals in Panama screening potential stroke patients.
XCath engineers were continuously testing the dedicated fibre connection, validating connectivity around the clock.
More than 60 physicians across 5 hospitals, all on standby, all united around one priority. The patient.
Then he arrived.
A man in his late 60s. Acute stroke symptoms. Brain imaging confirmed a large vessel occlusion of the left middle cerebral artery.
He was transferred to The Panama Clinic. NIHSS score of 21 on arrival. That score means a high likelihood of death or devastating disability without immediate intervention.
While he was being transferred, a process of around 15 minutes, the clinical team at the bedside were preparing the procedure room and connecting the Iris robot.
Nicole Cancelliere and local neurosurgeon Dr. Anastasio Ameijeiras Sibauste were with the patient throughout.
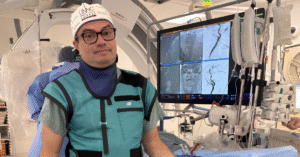
I was in Santiago. Two hundred kilometres away. At the controls.

I wrote afterwards that at that moment; the question was not whether the procedure could be performed. It was whether the technology was ready.
It was a significant moment. It was literally stepping off a precipice.
And Iris was ready!
I navigated the patient’s cerebral vessels remotely using the XCath Iris Surgical Robotic System.
I removed the clot. First pass. Complete reperfusion. No perceptible latency. No disruptions to the surgical workflow.
24 hours later his NIHSS score was 2. He was stable. He went home.
The President of Panama, José Raúl Mulino, received our team to mark the moment.
But the moment for me was not the ceremony. It was the patient going home.
It is one of the highlights of my career. And none of it happens without Nicole Cancelliere, whose leadership, precision, and dedication were instrumental in every step of this journey.
And without the extraordinary team at XCath, without Eduardo and Nicholas and every engineer who tested that fibre connection through the night, and without the 60 physicians across 5 hospitals who gave a week of their time to make sure that when this patient arrived, we were ready for him.
Geography is no longer a death sentence. That is what we proved.
And now we will expand this globally. Positioning robots in regional hospitals, in countries without neurosurgeons, in regions where today a stroke patient has no options. That is the mission.
THE SECRET NERD THAT LURKS WITHIN
Liz: That is an incredible story, and it just gives me goose pimples! That was a very brave patient and family, to try this. This is about saving lives and geography no longer being a death sentence.
Vitor, tell me about the other side of what you do in the lab. The side that is not robotics.
Vitor: Ah yes. I call it my nerdy side. And it has nothing to do with technology.
– I have 2 lines of research. One goes from the lab to the patient. New devices, robotics, imaging, translation. That is what people see.
– The other goes in the opposite direction. From the patient to the bench.
As I mentioned, I have conditions I cannot solve. Patients who come to me frustrated, sometimes with PTSD from years of not being understood, with symptoms the healthcare system has failed to explain.
Young women, often, with pulsatile tinnitus or intracranial hypertension or severe headaches that nobody fully understands yet.
Venous diseases. Lymphatic diseases. Genetic components.
A lot of uncertainty. No device is going to solve these.
I am at the very beginning with them, trying to understand the genesis of the conditions themselves. Gene expression. Genetic work. Basic science.
This line or this side of me traces directly back to Professor Lasjaunias. He was deeply academic. He always went back to first principles and understood everything from the ground up. I keep that with me.
People ask me how I manage such range across all of this. Robotics, AI, genetics, molecular biology. I tell them the honest answer.
I’m a nerd!
Some people watch Netflix. Some people play golf. I don’t do that… Instead, I read. I think. I build protocols. I organise thoughts. I spend a lot of time just thinking about unsolved clinical situations.
That is not a system. It is just how my mind works.
WHAT MAKES A YES
Liz: Vitor, you must get calls constantly from device wanting your involvement. What attracts you to a project?
Vitor: 2 conditions.
I only work with companies where I believe in the leadership first. That is always the starting point.
And the device or the project must be something I would use as a physician to treat my own patients.
Those are the 2 conditions.
If I would not use it clinically, I will not work on it. No exceptions.
Because I have the privilege of being able to choose, I choose based on those principles.
The field is still small enough that the people matter as much as the technology.
In every company I work with, I have people I get along with well, people who come with new ideas and projects, people who think the way I think.
I am lucky that in this field there are a lot of creative people building things rather than just talking about business. That is who I want to work with.
Liz: Vitor, you have worked with some incredible companies and you push the boundaries of what is possible constantly. Where is the line you will not cross?
Vitor: Patient safety. That is the line. And it never moves.
Every patient I see, every decision I make, I am balancing risk and benefit.
Sometimes life or death. We live at those extremes every day in this work. If the benefit is uncertain and there is risk, I am out.
Liz: Even if the patient says they are in?
Vitor: I am still out. That is not a rule I follow because I must.
It is a conviction. The patient in front of me is not always able to fully evaluate the risk they are accepting.
That responsibility sits with me, not with them.
Liz: That’s clear and that seems to be part of your North Star. Let’s move on and talk about NASA. I was surprised to read about the connection. How did that come about?
Vitor: Ah yes
Yes. I was invited to contribute as a scientific consultant on the validation of the formulation developed by Astreas.
They are a performance nutrition company working at the intersection of space science, human performance, and functional ingredients.
The work is about what happens to human performance under extreme conditions. Sleep deprivation. High stakes.
Environments where the limit is not theoretical but physiological. Like surgery.
What I know from surgery is this. Fatigue does not eliminate confidence. It distorts judgment while keeping the feeling of competence intact.
That is where mistakes take on the appearance of correct decisions. You feel certain. You are not.
Their Performance Spheres, functional chocolate formulated with clinically studied ingredients aims to support sustained focus and cognitive clarity.
It flew aboard NASA’s Artemis II mission as part of the crew’s food system.
The astronauts consumed them during the mission. As we know, they splashed down safely on April 10th.
For me it is not about space. It is about decisions that cannot fail. In surgery. In orbit. The conditions are different. The stakes are the same.
THE PILOT IN THE SURGICAL COCKPIT
Liz: So your research now includes space. What else, where else do you see this field going in the next ten years?
Vitor: I think the field will be completely different.
The pattern of our specialty has always been the same.
– An open surgical procedure becomes an endovascular procedure.
– That movement happened with aneurysms. It happened with stroke. It is now going to happen with other surgeries as well.
– VP (ventriculoperitoneal shunts) will become endovascular shunts.
– External neuromodulation will become internal.
– The shift in BCIs will continue moving from external toward internal and endovascular approaches.
– Venous diseases will be treated endovascularly. Local drug delivery to the brain will become possible in ways it simply is not today.
– And neuro-oncology. Most brain tumours, I believe, will eventually be treated endovascularly. Local delivery of drugs or radiation particles directly through the vessels. The blood brain barrier has always protected the brain from therapy as much as from disease.
The skull and the barrier prevent drugs and radiation from reaching tissue effectively from the outside. I believe we can change that from the inside and help patients who currently have almost no options.
I have a PhD student who has been working on endovascular approaches to glioblastoma and malignant meningioma for three years.
If all goes to plan, we do first in man before the end of this year.
Stroke and aneurysm will be around 30% of what we do. The other 70% will be procedures that barely exist in endovascular form today.
And most of it will be delivered using a robot. Not to replace doctors but to expand what doctors can do.
Precision. Consistency. Access.
The movement from open surgery to endovascular will now go from endovascular to robotic, and then from robotic to remote.
Every procedure. Everywhere.
I envision us working like pilots. Automation and AI as instruments. The surgeon still at the controls but with a much wider cockpit of options.
And patient-specific simulation, just as pilots use flight simulators to train and maintain competence.
That is a dream of mine that will absolutely become reality.
Liz: You mentioned BCIs. What are your thoughts about BCIs? Do you have any concerns there?
Vitor: No. None at all. I see BCIs entirely from the positive side.
Access to mobility. Access to communication. Recovery.
I am a big fan of neuromodulation and BCI is a natural extension of that.
We can stimulate the brain, diagnose diseases, monitor the brain, minimally invasively. That is all opportunity.
If people try to use it for enhancement beyond its clinical purpose, there will be consequences.
We saw the same with doping in sport in the 1980s. It got regulated. Consequences followed.
I am sure the same will happen here. There is always a limit. Someone will cross it and it will be more regulated.
I am not afraid of BCI from a medical perspective.
THIS WORRIES ME
Liz: So, if you’re not worried about BCI, is there anything at all that worries you about this field right now?
Vitor: My only real fear is that the fixed mindset voices in our specialty will be too loud for too long and delay the natural evolution of certain innovations.
Telesurgery is well accepted and adopted across almost every other surgical specialty.
In neurointervention it is still presented as a taboo.
And yet neurointervention is the specialty that arguably needs it most.
Time saves lives in stroke.
Distance costs lives. We are the ones who should be leading this conversation, not resisting it.
My hope is that with more awareness and more education, our colleagues will understand that it is far better to walk with technology than to be opposed to it.
Because technology does not stop. And it is far better to be a voice shaping it than to be left behind by it.
The train has left the station. You can be a bystander or an active contributor.

THE LOVE OF MY LIFE
Liz: I strongly agree with that, and Prof Dr Berhnard Meyer said exactly the same a few weeks ago to me. I want to ask you about what holds all of this together. Is there is something else?
Vitor: High performance medicine cannot be sustained without balance, integrity, and purpose.
Behind every protocol, every publication, every complex surgery, there is a structure that holds everything up.
For me that structure is faith, family, ethics, and team.
My wife Andrea has been with me since we were teenagers in Brazil.
She has followed me to France, to Switzerland, to Canada. She runs our home, our finances, our administration. She takes care of our three children, Alice, Pedro and Sarah, full time so that I can do what I do.
I can only work the way I work because she is who she is. Without her, none of this exists. This is the love of my life.
She is the key person in all of this journey. I think she likes to travel. I think she likes to explore. She has been a great, great partner through all of it.
When my children are awake and at home, I am with them. Present. We ski in the winter. We swim and bike in the summer. We cook together as a family.
Beef Wellington, grilled salmon, Brazilian barbecue with wagyu. I am learning the cello. I am learning Mandarin with my daughter.
This summer we are doing two triathlons together, the three kids and me.
And I am Christian. I pray. I read the Bible.
When people look at my path and ask how any of it was possible, how did I end up with Lasjaunias and then Moret, how did I end up in Canada with this career, I can only answer one way.
I ask God for blessing. Everything I have done and become I attribute to his grace and mercy.
I want to be known as someone blessed by God. For his glory as well.
A LEGACY
Liz: Last question and your last statement just prompted the thought, Vitor. What do you want to be remembered for?
Vitor: That is a question nobody has ever asked me before.
I’ll have to think about that for a moment.
I want to be known as someone passionate about my work. Passionate about people, about patients, about helping.
Someone who always went above and beyond and was never comfortable with the status quo.
Someone who always wanted to improve, to do better, to push further. Someone fair and honest.
And I want the next generation to carry this forward.
I am a tough teacher. I want my fellows to have the perfection of surgical technique, the attention to detail, the passion to study, and the curiosity that I have tried to bring to this work.
When I see them presenting in the conference sessions I am sitting in, I am very proud. Genuinely proud.
I want them to continue this legacy. Always thinking beyond.
Never paralysed by guidelines. Always safe, always fair.
And always making sure that whatever we develop reaches as many hands and as many patients as possible.
The evolution has to reach everyone. That is the whole point of all of it.

A FINAL THOUGHT
Vitor – a boy who wanted to build things, who ended up building the infrastructure to make stroke treatment available everywhere on earth. The engineer never left. He turned it to different problems.
He carries cases for years which he cannot yet solve.
Without Andrea none of this exists.
In a field that talks constantly about intelligence and innovation and disruption, he wants to be known as someone blessed by God.
I have spoken to a lot of remarkable people in this series. Vitor is another incredible one.

More to explore